Seniors often struggle with the use of telehealth due to challenges with technology and access. This article reviews effective solutions, including in-home assisted visits by care-team members who manage technology and enhance communication. Combining personal support, education and simplified tools can improve comfort, confidence, and telehealth engagement among older adults.

Telehealth has become a fundamental element in modern healthcare delivery. It provides convenience, improved access, and cost-effective options to traditional in-person visits to healthcare providers’ offices. However, while telehealth services have increased in popularity across many demographic groups, older adults, those who most likely stand to gain the most, remain significantly underrepresented in usage metrics. This disproportion originates from a combination of barriers: lack of digital literacy, physical and cognitive impairments, lack of familiarity with technology, and limited access to devices or reliable internet connectivity.
To fully appreciate the today’s situation, it is helpful to examine the historical path of telehealth in the United States. While the concept dates back decades, its use was largely limited to rural areas and specific specialties until the early 2010s. Even then, adoption was constrained by regulatory challenges, low reimbursement rates, and limited technological and operational infrastructure.
The pandemic was a major inflection point. Due to the high need of care, and low to no ability to access it, telehealth was transformed from a distant offering to a day-to-day necessity. CMS and other entities had to issue emergency policy waivers which enabled widespread use of video visits and phone calls and temporarily addressed licensure and payment barriers.
Dr. Samuel Lin, a health policy advisor and digital health consultant, notes, “COVID-19 didn't create the demand for telehealth, it exposed how urgent the demand already was. What it also showed is that without a human framework, technology alone can’t solve the access problem, especially for seniors.” This reflects the growing consensus among healthcare leaders: supporting staff like Medical Assistants (MAs) are the amalgams that make digital care functional and equitable.
According to the CDC’s 2021 National Health Interview Survey, only 43.3% of adults aged 65+ had used telemedicine services in the prior 12 months. On the other hand, telehealth was adopted by the younger populations, hitting 60% during the pandemic. This difference demonstrates a need to develop alternative solutions to help bridge the digital gap older adults are facing. The importance of expanding telehealth access to seniors cannot be overstated. As people age there is an increase in medical complexity, mobility limitations, and dependence on frequent medical visits. If utilized effectively, telehealth is excellently appropriate for it.
Interestingly, more than 75% of older Americans express a preference to remain in their homes as they age. To meet this goal, consistent medical oversight is crucial. Telehealth, with the help of in-home support, enables this wish while respecting seniors’ independence and preferences.
One of the most cost-effective, innovative and pragmatic solutions to help seniors engage in telehealth is the integration of MAs (or other care team supporters) into the virtual care experience. These professionals can provide hands-on assistance through in-home visits. These care givers can help with setting up devices, navigating telehealth platforms, and even staying with the patient during virtual appointments, providing comfort to those who may be in most need. MAs play a crucial role in eliminating technological friction and ensuring successful visit completion, increasing senior compliance.
By using this approach, not only will it address technological barriers but also improve the emotional experience for seniors. Sharing this important moment with a friendly and trained assistant can significantly reduce anxiety and increase a senior's willingness to participate in telehealth services. Moreover, in many cases, MAs also act as scribes, documenting the interaction, freeing providers to focus on care delivery, and ensuring no important details are missed.
The financial implications of improving telehealth access for seniors are also significant. The National Committee for Quality Assurance (NCQA) reports that telehealth has the potential to replace up to $250 billion of annual U.S. healthcare spending. This substitution stems from reduced hospital admissions, fewer emergency department visits, and more consistent chronic condition management. Adding MA support into this equation enhances efficiency by ensuring that appointments run smoothly, technology works properly, and patients are better prepared.
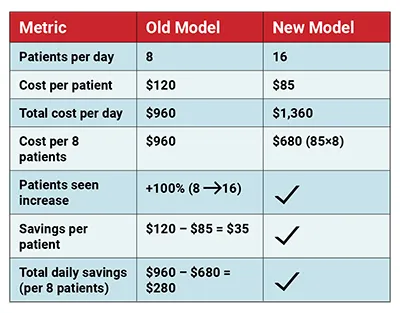
To analyze the financial gains deeper, we have created a simulation. An average primary care provider’s hourly rate is $120 per hour, while an average MA’s hourly rate runs around $25 for certified MAs. Assuming that a patient’s visit takes 30 minutes and there are another 30 minutes spent commuting from a patient’s home to the next, the model proposes having a ratio of 2 MAs per PCP to avoid time wasted from PCP. In this simulation, the PCP stays in a fixed location doing the televisit, while the MAs do the in-home visits. Adopting this model saves close to 30% of the total cost and doubles the number of patients that can be seen per provider. (see table below)
An interesting example of this potential comes from a Texas based group’s data during the COVID-19 pandemic. Their analysis showed that Medicare beneficiaries, most of which are 65 and older, accounted for 23.5% of all telehealth users. In regions where patients received technical support, that figure increased markedly.
Hospital systems and health plans that have implemented “tele-home-care” models, often incorporating MA-like roles, have seen tangible clinical, financial and emotional improvements for older adults. For example, programs focused on managing chronic diseases like heart failure and diabetes have demonstrated a 65% reduction in avoidable hospital admissions. These outcomes are achievable because there is a more consistent check-in process which allows providers to intervene early, adjust medications, or offer guidance before an acute situation occurs. MA support ensures that these virtual connections actually happen, and seniors don’t miss the opportunity to contact their providers when needed due to fear of technology.
A crucial and often underappreciated and undermeasured aspect of MA-supported telehealth is its role in enhancing communication. Seniors often struggle to fully understand or retain complex medical information during visits. With a trained assistant present, instructions can be repeated, notes can be clarified, and follow-up steps can be documented clearly. This added layer of communication reduces confusion and increases adherence to treatment plans and medications.
Another example of the successful implementation of this program is a Midwest-based ACO which piloted an initiative where medical assistants conducted monthly home visits to provide telehealth support to high-risk Medicare patients. Over a 9-month period, the program reported a 12% increase in appointment adherence, a 20% drop in 30-day readmissions, and a net cost savings of $1,100 per patient per year. These results emphasize not only the clinical but also the financial value of incorporating dedicated support staff into the telehealth ecosystem.
In order to scale this model nationally, several strategic operational steps must be considered. First, medical assistants need specialized training in digital health tools, such as EMR (electronic medical records) and others, privacy compliance (HIPAA), and the nuances of senior care. Second, healthcare organizations must allocate resources to allow for in-home MA support for telehealth visits. Third, public and private payers should recognize and reimburse these services as essential components of care delivery.
Policy recommendations from advocacy organizations like the American Hospital Association and NCQA suggest that the reimbursement models for telehealth be updated to include not only provider time but also the support roles that make telehealth successful. This is particularly relevant for seniors on fixed incomes who rely on Medicare or Medicaid. Pilot programs and value-based care contracts are ideal settings to introduce these expanded service models and evaluate their effectiveness.
From a human perspective, the impact of a supportive MA presence can be profound. Patients report feeling more confident and more connected to their providers, even from the comfort of their own homes. In addition, supporting seniors in telehealth also alleviates caregiver burden and burnout. Many adult children of aging parents serve as informal caregivers and often struggle to balance their own responsibilities. MA-supported telehealth helps ease this tension by ensuring that care can continue without relying solely on family members for logistics or technology setup.
For policy makers and payer organizations, the message should be clear and consistent: investing in care extenders such as medical assistants drive success not just in care delivery but in system-wide efficiency. Incentive structures should be adapted to reimburse collaborative, team-based telehealth models.
Ultimately, the future of telehealth will not be driven solely by AI, apps and algorithms, but by thoughtful integration of human-centered support. As we continue to evolve in our healthcare delivery models, ensuring that no one is left behind (especially our senior population) must remain a golden rule. Medical assistants offer a scalable, effective, and deeply human way to make that gravision a reality. Their role is not just helpful but necessary.
Looking ahead, incorporating data from MA-assisted telehealth visits into population health management systems could provide even more value. By tracking outcomes, engagement levels, and costs, health systems can optimize care models and identify the most effective interventions. This could pave the way for predictive analytics that tailor outreach to those at highest risk of disengagement, and therefore, worse outcomes.
As we move into a new era of value-based care, the stakes are clear. Health outcomes, patient experience, and financial performance are all interlinked. Solutions like MA-assisted telehealth don’t just check one box, they simultaneously improve quality, equity, and efficiency. For this reason, healthcare executives, payers, and policymakers alike should view investment in such models not as a luxury, but as a strategic imperative.
References
1. Centers for Disease Control and Prevention (CDC). (2022). Telemedicine Use Among Adults: United States, 2021. National Center for Health Statistics, Data Brief No. 445.
Retrieved from: https://www.cdc.gov/nchs/products/databriefs/db445.htm
2. National Committee for Quality Assurance (NCQA). (2020). Taskforce on Telehealth Policy: Findings and Recommendations.
Retrieved from: https://www.ncqa.org/programs/data-and-information-technology/telehealth/taskforce-on-telehealth-policy/taskforce-on-telehealth-policy-findings-and-recommendations-telehealth-effect-on-total-cost-of-care/
3. Carenet Health. (2020). Telehealth Usage by Insurance Type: COVID-19 Consumer Insights Report.
Retrieved from: https://carenethealthcare.com/young-adults-using-telehealth-more-older-and-lower-income-americans-slower-to-adopt-covid-19-report/
4. American Hospital Association (AHA). (2020). Fact Sheet: Telehealth.
Retrieved from: https://www.aha.org/fact-sheets/2020-02-07-fact-sheet-telehealth
5. Stanford University School of Medicine. (2021). Digital Health: Evaluating AI in Healthcare. Course Materials.
6. Pew Research Center. (2021). Older Adults and Technology Use. Retrieved from: https://www.pewresearch.org/internet/2021/04/07/older-adults-and-technology-use/
7. Lam, K., Lu, A. D., Shi, Y., & Covinsky, K. E. (2020). Assessing Telemedicine Unreadiness Among Older Adults in the United States During the COVID-19 Pandemic. JAMA Internal Medicine, 180(10), 1389–1391.
https://doi.org/10.1001/jamainternmed.2020.2671
8. Wildenbos, G. A., Peute, L., & Jaspers, M. (2019). Barriers in using mobile health apps and devices in the aging population. mHealth, 5(41). https://doi.org/10.21037/mhealth.2019.09.02

Silvana Fischman, DDS(Intl), MHA, CRC brings 20+ years of executive leadership in clinical operations, having built, scaled, and optimized initiatives across primary and specialty care models. As the founder of Chai Class Consulting, Silvana partners with healthcare organizations to deliver data-driven strategies, streamline operations, and improve efficiency, cost, and outcomes.
