The integration of AI into radiology enhances diagnostic imaging by identifying, prioritizing, classifying, and quantifying critical, non-critical, and incidental findings. Clear workflows and clinical pathways are needed to manage these findings while considering both FDA clearance and patient consent. Implementing AI requires updated healthcare protocols to address ethical, legal, and clinical concerns. This paper outlines workflow and management pathway categories for AI-generated findings, highlights Human Intervention's (HI) role, discusses procedural requirements, and proposes a systematic approach to these challenges in practice.

Artificial intelligence (AI) has transformed healthcare, particularly in radiology, enhancing diagnostic accuracy, improving patient care, and reducing errors. AI algorithms are being used not only for image analysis but also for non-diagnostic tasks such as workflow optimization, scheduling, prioritization, and quality assurance. AI can optimize the radiology workflow by automating triage and refining report generation, rapidly sorting, and prioritizing radiological studies such as CT scans and MRIs according to urgency, drawing attention to critical cases that require immediate attention. This includes automating triage and prioritizing cases, which ensures critical conditions like stroke, hemorrhage, and malignancy are addressed quickly. AI, especially natural language processing (NLP), helps reduce repetitive tasks, alleviating radiologist burnout.
For AI to work optimally in clinical settings, it must be seamlessly integrated into existing radiology systems. This requires clear workflows that dictate how these findings are managed, considering both FDA clearance and patient consent, and local validation of AI models, as the accuracy of algorithms can vary due to differences in imaging equipment, protocols, and patient populations. The American College of Radiology (ACR) emphasizes the importance of local validation and human intervention (HI) to ensure AI algorithms perform effectively in specific clinical environments, maintain accuracy over time, and address any variations, thereby safeguarding patient safety and care quality. Furthermore, ensuring patient confidentiality and informed consent (IC) is crucial as AI’s “black box” nature can obscure decision-making processes, requiring transparency and safeguards to protect patient autonomy.
During the rollout of FDA-cleared AI imaging algorithms in a large academic healthcare system, we encountered challenges that required the creation of new workflows and personnel roles. This paper provides insights into integrating AI in radiology, highlighting the need for human intervention to maintain accuracy and regulatory compliance. We outline workflows for managing AI-generated findings, the need for new roles to improve operational efficiency, and resources required for comprehensive management. Additionally, we explore the regulatory and ethical complexities of AI in medical imaging, emphasizing patient engagement and the importance of clear definitions in AI applications.
AI enhances diagnostic precision, reduces workload, and enables radiologists to focus on complex cases. New roles, such as advanced practice providers (APPs) imaging specialists and clinical care coordinators (CCCs), improve result communication and patient management, advancing healthcare delivery.
We employed a phased approach, beginning with IRB-approved pilot projects. We analyzed infrastructure, staffing, and finances to ensure feasibility, adjusting strategies based on real-world feedback.
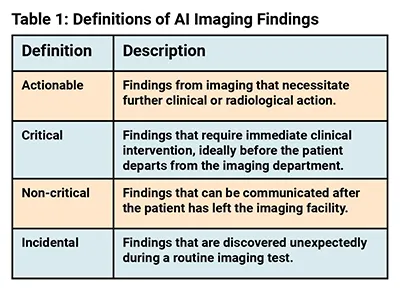
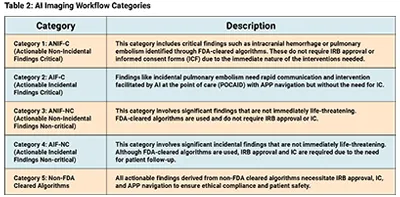
Clear definitions and workflow categories streamline AI integration (Tables 1 and 2). Categorizing findings as "actionable," "critical," "non-critical," or "incidental" ensures appropriate clinical responses while addressing regulatory and ethical complexities.
Strict oversight is required, especially for non-FDA-cleared algorithms. The IRB ensures compliance, while informed consent (IC) ensures patients understand AI’s role in their care, particularly for findings requiring further medical intervention.
In Florida, APPs, including ARNPs, PAs, and physicians, are required to deliver imaging results instead of nurses. APPs manage AI-generated findings, stabilizing patients and providing critical care in emergencies (i.e., point-of-care AI deployment (POCAID) Category 2). For non-critical findings (i.e., POCAID Category 4), APPs coordinate patient engagement and follow-up.
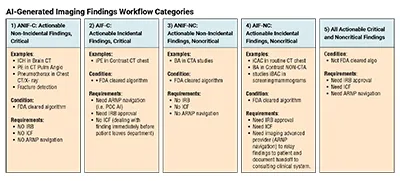
Imaging APPs are needed to convey findings in Categories 2, 4, and 5. Category 2 involves critical incidental findings needing immediate action, Category 4 involves actionable incidental findings that are non-critical but require patient follow-up, and Category 5 involves findings from non-FDA cleared algorithms, requiring careful navigation for compliance and safety.
For Categories 1 and 3, nurse practitioners are not required to convey findings. Category 1 includes critical actionable non-incidental findings requiring immediate clinical intervention, typically managed directly by the attending radiologist or emergency medical personnel. Category 3 includes non-critical findings that can be communicated later through follow-up, without requiring direct involvement of APPs. In these categories, the primary focus is on timely response rather than extended patient engagement.
In Categories 1 and 3, non-incidental findings require different medical responses than incidental findings, reducing the need for APP involvement. For Categories 1 and 3, APPs are not required to convey findings to patients due to their nature. Category 1 includes critical actionable non-incidental findings, requiring immediate clinical intervention typically by the attending radiologist or emergency personnel, eliminating the need for APPs. These findings also don’t require informed consent due to their urgency.
Conversely, Category 3 consists of non-critical non-incidental findings, which can be communicated after the patient leaves the facility the non-urgent nature allows follow-up by various clinical staff, not requiring APPs. Informed consent is typically unnecessary, as these findings are addressed within standard care procedures without the introduction of experimental or unapproved diagnostic tools.
The role of CCCs has expanded to serve as a liaison between APPs, physicians, patients, and other healthcare providers, ensuring efficient care management. At our institution, CCCs monitor patient dashboards for timely alerts, focusing on the POCAID pilot to ensure provider communication and patient safety. When a positive alert occurs, the technologist, CCC, and onsite APP coordinate with the radiologist to confirm findings, communicate with providers, and plan dispositions. CCCs supervise dashboard alerts to ensure no alerts are missed and true positives are reconciled. We track alerts for quality monitoring and are reassessing workflows based on radiologist feedback on alert intervals.
Web-based patient follow-up manager platforms are key tools for integrating HI and AI-enhanced radiology workflows. They streamline care by coordinating between providers, APPs, CCCs, and patients, ensuring proper management of AI findings. These platforms enable timely follow-up on both critical and non-critical findings, reducing missed diagnoses and improving care quality. They also help maintain ethical compliance and patient autonomy by tracking consent for AI technology use.
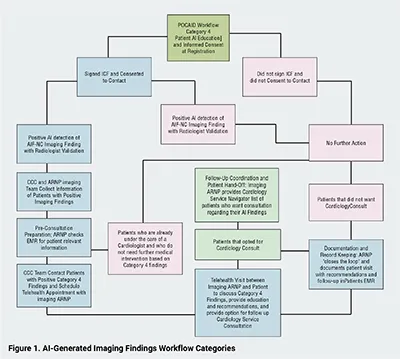
The incorporation of AI into medical imaging necessitates a robust process for notifying patients about AI’s role in their imaging evaluations. For FDA-cleared AI, written consent is not mandatory, but patients must be informed. In IRB-approved pilot studies, consent is encouraged for Category 4 findings and required for Category 5 findings due to experimental AI technology use.
AI-enhanced radiology workflows categorize findings to ensure appropriate patient management and safety (Tables 1 and 2). Categories differentiate between actionable, critical, non-critical, and incidental findings, tailoring responses based on urgency and regulatory requirements (Figure 1). Actionable findings necessitate further action, while critical findings demand immediate intervention, and non-critical and incidental findings, which can be communicated after the patient leaves.
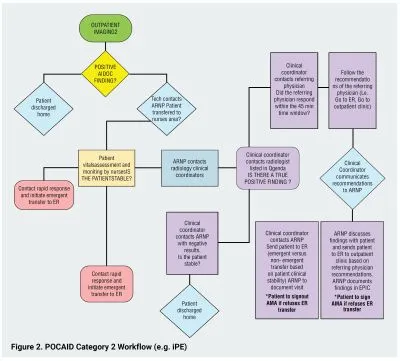
For Category 2 critical incidental findings (i.e., incidental pulmonary embolism (iPE)), AI alerts trigger a coordinated emergency response via POCAID (Figure 2). Patients remain in the imaging center under APP supervision while radiologists validate AI findings. Confirmed cases are managed promptly, stabilizing patients before ER transfer.
For Category 4 actionable incidental but non-critical imaging findings (i.e., incidental coronary artery calcification scores (iCAC), APPs and CCCs use AI-driven tracking tools to coordinate follow-ups (Figure 3).
Routine AI vendor meeting facilitated the deployment of an FDA-cleared coronary calcium scoring algorithm, forming the basis for a preventive care workflow. This initiative is expected to expand into additional areas like breast calcifications.
The POCAID Category 2 workflow addresses critical incidental findings, specifically specifically PEs detected during CT scans not primarily targeting PE. When AI identifies an iPE, an emergency response is triggered (Figure 2). A radiologist verifies the finding while the patient remains in the imaging facility for continuous care.
Imaging APPs stabilize unstable patients and coordinate necessary interventions, from anticoagulation therapy to invasive procedures. CCCs facilitate communication between the patient’s provider and ER teams for immediate response alignment. If ER transfer is needed, stabilized patients are transported by ambulance, ensuring the receiving team is fully informed for prompt care. This streamlined approach minimizes time from detection to treatment, enhancing patient outcomes.
We plan to initiate an IRB-approved pilot program at an outpatient imaging center to track AI-generated iCAC scores. After radiologists finalize reports, ARNP imaging teams use an AI-based management tool to monitor patients with moderate- to high-risk scores (Figure 3). APPs and CCCs collaborate to contact patients, discuss results, and arrange follow-ups.
CCCs manage logistics and facilitate patient-provider interactions, while APPs oversee clinical interpretation and direct communication. This ensures timely, high-quality care. The AI-based tracking tool queries the Epic system to determine if patients are already receiving cardiac care. Those meeting criteria—such as being on statins or under cardiology care—are removed from the workflow, allowing APPs to focus on new cases.
We selected all moderate to high iCAC patients not on statins to be entered into the worklist as “Identified.” APPs offers these patients a cardiology consultation, which is recorded in our electronic medical record (EMR), and the patient is moved to “Scheduled.” The tool auto-closes when a cardiologist’s report is generated, automatically moving the patient to “closed” once the report is available.
Following legal advice, it was crucial to clearly communication clinically significant AI-generated findings (specifically the iCAC score) to patients after radiologists completed their reports, with documentation of the patient’s understanding. This underscored the need for an APP follow-up visit. We aim to expand this workflow system-wide, starting with this pilot.
AI integration requires investment in technology, training, and staffing. APPs and CCCs play critical roles in managing AI findings, necessitating specialized training.
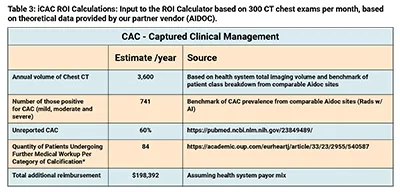
For our IRB workflow pilot, we presented a theoretical business plan based on published data, estimating downstream revenue from increased specialist referrals. For instance, POCAID Category 4 iCAC workflow estimates an average of 148 wRVUs per month, generating substantial revenue (Table 3). Vendor ROI projections suggest AI could identify 84 missed coronary interventions annually, adding $198,000 in revenue.
These financial models justify funding for IT infrastructure, compliance measures, and personnel required for sustainable AI implementation.
Integrating AI into radiology requires structured workflows to manage AI findings while ensuring regulatory compliance and patient safety. Clear definitions, protocols, and transparent patient communication facilitate successful implementation.
Our framework can be refined with technical AI descriptions, case studies, economic impact analyses, and a stronger focus on patient experience. Long-term monitoring strategies are needed to address AI biases and reliance on technology.
This paper establishes foundational AI-enhanced workflow strategies. Future research will explore challenges, advancements, and ethical considerations in AI-integrated radiology.
Although we did not receive direct funding from AIDOC and have no disclosures, AIDOC has committed to reimbursing our department for the IRB submission costs.
References
1. Najjar R. Redefining Radiology: A Review of Artificial Intelligence Integration in Medical Imaging. Diagnostics (Basel). 2023 Aug 25;13(17):2760. doi: 10.3390/diagnostics13172760. PMID: 37685300; PMCID: PMC10487271.
2. Wiggins WF, Magudia K, Schmidt TMS, O'Connor SD, Carr CD, Kohli MD, Andriole KP. Imaging AI in Practice: A Demonstration of Future Workflow Using Integration Standards. Radiol Artif Intell. 2021 Oct 27;3(6):e210152. doi: 10.1148/ryai.2021210152. PMID: 34870224; PMCID: PMC8637229.
3. Ranschaert E, Topff L, Pianykh O. Optimization of Radiology Workflow with Artificial Intelligence. Radiol Clin North Am. 2021 Nov;59(6):955-966. doi: 10.1016/j.rcl.2021.06.006. PMID: 34689880.
4. Tadavarthi Y, Makeeva V, Wagstaff W, Zhan H, Podlasek A, Bhatia N, et al.. Overview of noninterpretive artificial intelligence models for safety, quality, workflow, and education applications in radiology practice. Radiol Artif Intell 2022; 4(): e210114. doi: 10.1148/ryai.210114
5. European Society of Radiology (ESR) . Current practical experience with artificial intelligence in clinical radiology: A survey of the european society of radiology. Insights Imaging 2022; 13(): 107. doi: 10.1186/s13244-022-01247-y
6. Allen B, Dreyer K, Stibolt R, Agarwal S, Coombs L, Treml C, et al.. Evaluation and real-world performance monitoring of artificial intelligence models in clinical practice: Try it, buy it, check it. J Am Coll Radiol 2021; 18: 1489–96. doi: 10.1016/j.jacr.2021.08.022
7. Hosny A, Parmar C, Quackenbush J, Schwartz LH, Aerts HJ. Artificial intelligence in radiology. Nat Rev Cancer. 2018;18:500-510. doi: 10.1038/s41568-018-0016
8. https://aicentral.acrdsi.org/
9. https://www.acrdsi.org/DSI-Services/AI-Central/Transparent-AI
10. https://www.acr.org/Advocacy-and-Economics/Advocacy-News/Advocacy-News-Issues/In-the-May-11-2024-Issue/ACR-Provides-Insights-on-AI-Oversight-Use-and-Innovation-in-Response-to-Congressional-RFI
11. Goisauf M, Cano Abadía M. Ethics of AI in Radiology: A Review of Ethical and Societal Implications. Front Big Data. 2022 Jul 14;5:850383. doi: 10.3389/fdata.2022.850383. PMID: 35910490; PMCID: PMC9329694.
12. Geis JR, Brady AP, Wu CC, Spencer J, Ranschaert E, Jaremko JL, Langer SG, Borondy Kitts A, Birch J, Shields WF, van den Hoven van Genderen R, Kotter E, Wawira Gichoya J, Cook TS, Morgan MB, Tang A, Safdar NM, Kohli M. Ethics of Artificial Intelligence in Radiology: Summary of the Joint European and North American Multisociety Statement. Radiology. 2019 Nov;293(2):436-440. doi: 10.1148/radiol.2019191586. Epub 2019 Oct 1. PMID: 31573399.
13. https://www.lbmc.com/blog/physician-work-rvu-increases-in-2023/
14. https://www.bnncpa.com/resources/2021-physician-fee-schedule-changes-and-the-impact-to-wrvu-physician-compensation-agreements/
Dr. Jean Jose is a professor of radiology and Associate Vice Chair of IT at the University of Miami Miller School of Medicine, specializing in musculoskeletal radiology. He has published extensively on interventional and diagnostic MSK imaging techniques and AI applications, focusing on improving diagnostic accuracy, AI-driven workflows, and patient outcomes.

Dr. Chloe Issa is a resident physician pursuing her residency in Diagnostic and Interventional Radiology. She contributes to research on the ethical implications of AI in healthcare, advocating for patient-centered approaches in technology integration.

Dr. Thiago Braga is an assistant professor and Vice Chair of IT in the Department of Radiology at the University of Miami, specializing in ER radiology. With a background in IT and AI, he contributes to projects aimed at enhancing workflow efficiency and diagnostic precision through AI in medical imaging.
Dr. Jose Net is an associate professor of radiology, division director breast imaging, and Vice Chair of Clinical Operations at the University of Miami. He is at the forefront of integrating AI tools to improve diagnostic accuracy in breast imaging, particularly for the early detection of breast cancer.

Dr. Fernando Collado Mesa is a professor of radiology and Associate Vice Chair of AI Ethics and Research at the University of Miami, specializing in breast imaging. He leads initiatives to incorporate AI into mammography and AI governance, enhancing the detection and management of breast cancer through advanced imaging technologies.

Steven Falcone, MD: Dr. Steven Falcone is a professor of radiology, neuroradiologist and Associate Chair of the Department of Radiology at the University of Miami. He has been instrumental in implementing AI technologies in clinical workflows, improving efficiency and patient care in radiology practice.

Ioannis Chatzizisis, MD, PhD: Dr. Ioannis Chatzizisis is a professor of cardiovascular medicine and radiology, and Division Director of Cardiology Services at the University of Miami. With expertise in computational and interventional cardiology, he develops AI-driven models to predict and manage cardiovascular diseases, bridging the gap between radiology and cardiology.

Alexander McKinney, MD: Dr. Alexander McKinney is a professor of radiology and Chair of the Department of Radiology at the University of Miami. With extensive experience in neuroradiology, IT, AI, and informatics, he advocates for the integration of AI in radiology education and clinical practice, preparing the next generation of radiologists.
