Section I: Charting the Rise of AI in Diagnostic Imaging
Interview with: James Holroyd, MD, Blackford Analysis
Q: James, let’s start at the beginning—how did early AI in radiology get started?
James Holroyd: The first FDA-cleared application for assistive computer-aided detection (CAD) was R2’s ImageChecker for mammography in 1998, developed to assist radiologists in identifying suspicious regions on screening mammograms. By the early 2000’s, there were over 1,000 ImageChecker systems installed worldwide, providing CAD assistance for millions of mammograms.
That device helped lay the groundwork for regulatory pathways to combining AI, clinical evidence, and medical device review—a significant step toward modern AI in medicine.
Q: How has AI adoption in diagnostic imaging evolved since then?
James Holroyd: Once ImageChecker demonstrated clinical feasibility and commercial viability, the field expanded into broader computer-aided detection and diagnosis. Over the past decade, technology advancements in the field of Artificial Intelligence (AI) through improvements in computing power and algorithm development technologies, such as deep learning, have revolutionised how medical imaging data can be interpreted. Today, the FDA has cleared over 1,350 AI-enabled devices across clinical specialties, and radiology still accounts for roughly 77% of those clearances.
Health systems are moving beyond point solution AI applications to more scalable enterprise solutions that support multiple specialties, providing image analysis and detection, workflow triage and prioritisation, image quality, treatment planning, reporting and documentation support.
This has driven the need for AI Orchestration Platforms that support the enterprise and host a variety of AI applications from different vendors with varied deployment models. Platforms simplify the integration of AI into PACS, RIS, and EHR workflows, and manage deployment, monitoring, security, and governance, which enables hospital systems to adopt and scale AI more efficiently.
Breakdown: FDA-Cleared AI Devices by Specialty (approximate proportions)
Based on data from The Physician AI Handbook, Appendix D
• Radiology – ~77%
• Cardiology – ~8%
• Pathology – ~4%
• Ophthalmology – ~3%
• Dermatology – ~2%
• Others (neurology, internal medicine, GI, psychiatry, etc.) – ~6%
These figures reflect not only historical momentum in imaging, but also the robust clinical evidence, structured workflows and change management that support AI integration and adoption.
Q: Why has radiology led the way in FDA-cleared AI tools?
James Holroyd: Radiology was already a highly digitised specialty well before AI became practical. Images were captured, stored, and managed digitally, creating rich datasets ideal for machine learning. Pathway clarity, clinical need for efficiency and accuracy, and strong vendor investment also helped drive radiology to represent the majority of AI clearances.
AI also arrived when a “perfect storm” of factors was challenging the specialty of radiology. Medical Imaging volumes were increasing faster than the number of radiologists entering the field. As an example, between 2005 and 2019, there was an 80% increase in imaging study volumes, as well as a 4x increase in images produced in CT and MRI studies from 2005 to 2020. With growing volumes and a 30-40% shortage of practising radiologists globally, resources are stretched. In fact, 53% of radiologists report that burnout is their biggest concern for the future of radiology. Many radiology departments, as well as other specialties such as cardiology, are looking to AI to support the growing workload and cognitive load associated with these challenges.
Section II: The Emergence of On-Edge AI in Real-Time Clinical Use
Interview with: Devon Bream, MPH, FACHE, BARCO Healthcare
Q: What is “on-edge AI,” and why is it emerging now?
Devon Bream: On-edge AI refers to algorithms and models running locally at the point of care—either directly on devices such as imaging scanners, clinical monitors, or bedside platforms—rather than solely in cloud infrastructure. This approach dramatically reduces latency and allows real-time decision support, which is becoming essential for time-critical clinical environments.
The recent emergence of these algorithms is due in large part to the FDA's 2021 released its “Artificial Intelligence/Machine Learning Based Software as a Medical Device Action Plan”. This plan outlined its steps, which eventually led to the current 2025 FDA draft guidance. Additionally, CMS provided a reimbursement pathway in its 2025 reimbursement schedule, which ultimately provided a way for AI developers to develop revenue models. The combination of these recent actions has created exciting clinical development activities in the healthcare sector, but in particular in point-of-care settings.
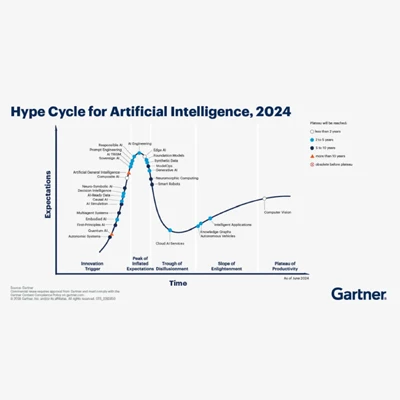
However, the excitement needs to be balanced until true ROI’s and adoption occurs similar to the experience James shared with radiology. Following the Gartner curve, we are clearly in the peak of expectations stages as illustrated below:
Q: How is on-edge AI being used in clinical settings today?
Devon Bream: We’re seeing on-edge AI assist in real-time surgical navigation, intraoperative imaging feedback, continuous patient monitoring, and ICU support systems. By processing data locally, clinicians get rapid insights without reliance on connectivity or remote servers, improving responsiveness in urgent care scenarios.
As you see with the data referenced from The Physicians AI Handbook above, the next fastest area of AI application growth, behind radiology, is cardiology. This is particularly interesting as the clinical interventions in cardiology stand to greatly benefit from AI decision support, guidance, and clinical efficiency.
Q: What challenges do hospitals face when adopting on-edge AI?
Devon Bream:
• Key considerations for administrators and IT leaders are similar to those addressed in radiology, including: Integration with existing clinical systems: Seamless data flows between devices, EHRs, and workflows.
• Security and privacy: Local processing must meet HIPAA and cybersecurity standards.
• Dealing with multiple platforms is required to run individual AI applications at the point of care. Whereas radiology has benefited from post-image processing, the real-time demands of on-edge solutions require proper platforms to host multiple AI applications easily accessed with proper computing power.
• Validation and support: Ensuring AI outputs are reliable and maintain up-to-date models as clinical practices evolve.
• Workforce readiness: Training clinicians to interpret and act on algorithmic insights.
Looking Ahead: A Shared Vision for AI in Healthcare
Q: Where do you see AI in healthcare heading over the next decade?
James Holroyd: AI will evolve from assistive tools supporting single tasks to become a multimodal, integral component in clinical workflows—supporting diagnosis, triage, risk prediction, planning, and guidance. AI will move from “What is on the scan?” to “What does this mean for this patient, right now?” As models mature and data ecosystems become more interoperable, AI will support broader, evidence-based care decisions.
Multimodal AI represents the next major evolution in radiology, moving beyond image only algorithms to systems that integrate imaging, clinical data, text, and time based information. This will improve diagnostic relevance, reduce false positives, and better support complex tasks such as triage, follow up recommendations, treatment response assessment, and multidisciplinary decision making.
The strategic value of multimodal AI lies less in incremental accuracy gains and more in workflow efficiency, prioritisation, and clinical decision support at scale. Key challenges remain around data integration, governance, explainability, and regulation, but the direction is clear: multimodal AI shifts radiology AI from “pattern recognition” to context aware clinical support, aligning technology more closely with how care is actually delivered.
Devon Bream: I envision AI that is deeply integrated at the point of care. On-edge systems will help teams function faster and smarter while enhancing safety and efficiency. But leaders must prioritise ethical deployment, governance, proper infrastructure and platform deployment, and clinician–AI collaboration.
Q: What advice would you give to healthcare leaders preparing for this future?
James Holroyd: Understand what AI can do across your health system; where it can add value and where it will require oversight. Invest in enterprise-wide solutions that scale efficiency, build connectivity across specialisms, and drive adoption across the health system.
Devon Bream: Focus on change management—embracing AI isn’t just a technology swap; it’s transforming care delivery. Proactive governance and clear metrics for success will be critical.
Conclusion
From the first mammography-focused AI in 1998 to an ecosystem with over 1,350 FDA-cleared tools, artificial intelligence has matured into a central pillar of clinical innovation. Radiology’s leadership remains clear, but emerging on-edge AI promises to push boundaries beyond imaging and into real-time patient care, requiring thoughtful integration, clinical validation, and strategic vision from healthcare leaders.
References:
[1] Y.-C. Peng et al. Radiologist burnout: Trends in medical imaging utilisation under the national health insurance system with the universal code bundling strategy in an academic tertiary medical centre. European Journal of Radiology 157 (2022) 110596
[2] Siewert et al. Summary of the 2023 ACR Intersociety Meeting. Journal of the American College of Radiology Volume 22 - Number 1 - January 2025. 30-40% global shortage in radiology, cardiology + workforce
[3] Radiology Unlocked: The Global Radiologist Report 2025.


