Cardiovascular Imaging Services is one of the fastest growing areas of the healthcare market. The traditional model of siloed imaging departments is being disrupted as the volume and complexity of cases increase. Multimodality Cardiovascular imaging practice, training, and service line organisation must evolve to meet the demands of the current healthcare environment.

As technology progressed, various CVI modalities were developed in the 20th century. These included M-mode echocardiography (echo) in 1953 (Edler and Hertz), single photon emission Computed Tomography (SPECT) in 1963 (Kuhl and Edwards), cardiac computed tomography (CCT) in 1972 (Hounsfield), Positron Emission Tomography (PET) in 1973 (Phelps and Hoffman), Cardiac Magnetic Resonance (CMR) in 1973 (Lauterbur), and the important hybrid field of Structural Heart Disease Imaging (SHDI) in 2007 (Hahn, Leipsic, Leon). Due to the sequential nature of the CVI modalities that were developed at different times and in different locations with different technological factors, each progressed separately. This created 4 general categories of CVI: 1) Echocardiography, 2) Nuclear Cardiology (SPECT + PET), 3) CMR, and 4) CCT It was rare that a physician was an expert in more than 1 of these CVI modalities.
The rapid evolution of the field of structural heart disease and SHDI demonstrated clearly that expertise was required in multiple CVI modalities to facilitate pre-procedural planning and intra-procedural case guidance. Multimodality Imaging (MMI) expertise is becoming more common for new trainees and is routine for those focused on imaging practice.
Cardiovascular Imaging (CVI) is one of the fastest growing areas of the healthcare market. From 2013 to 2022, United States Medicare data have shown that PET, CMR, and CCT volumes have more than doubled, tripled, and quadrupled, respectively, whereas echo volumes have slightly declined and SPECT volumes have declined by 1/3. In total, given that echo and SPECT are the highest volume modalities, a slightly decline in total CVI procedures has occurred. However, the projections for CVI moving forward estimate a compound annual growth rate (CAGR) of 6-8% moving forward, with a higher CAGR expected from CCT and PET as compared to other modalities. Cardiologist billing for the combination of CCT, CMR, and PET has decreased from 73.6 to 58.6% of the procedures from 2013 to 2022, while Radiologist billing has increased from 19.7% to 35.2%.
Both Cardiologists and Radiologists are currently facing worsening national supply-demand mismatch within their fields. Cardiologists in training receive minimal education in the newer CVI modalities of CCT, CMR, and PET. To become proficient in these, extra training beyond the 3 years of Cardiovascular Diseases Fellowship is usually required. In most hospitals around the United States, CCT and CMR programs are run within the Department of Radiology which can further limit and complicate training for Cardiology Fellows. As CVI fellowships are not accredited by the Accreditation Council of Graduate Medical Education, CVI is not a universally recognized subspecialty of Cardiology. While the American Board of Radiology certifies Radiologists to read CVI studies, the training and exposure to cardiovascular anatomy, physiology, and clinical cardiovascular implications may be limited during General Radiology Residency. As CVI study acquisition and interpretation is more technically challenging and time consuming than the vast majority of Radiology non-CVI studies, image quality and turnaround times may suffer.
Reimbursement is another challenge for CVI, as noninvasive diagnostic studies are reimbursed at a lower rate than invasive diagnostic studies and therapeutic interventions. The facility fee and read of a coronary CCT for example, is reimbursed at a few hundred dollars whereas an invasive diagnostic angiography without intervention would be reimbursed ~10 fold higher for a similar time of assessment. Many cardiologists are also encouraged to participate in structural heart disease imaging (SHDI) due to the massive manpower demands of the field, and are then exposed to radiation and orthopedic risks which are incongruous with salary. Reimbursement based limitations in the salary of an imaging physician and occupational risks lead to lower recruitment into the field. Practice patterns in both Cardiology and Radiology result in limited dedicated time to read CVI studies. The above factors may further lead to job dissatisfaction.
Due to the rapid growth of CVI, training, quality assurance, and throughput are major challenges. While attempts are being made to enhance training quality and increase the number of training slots to produce more Cardiologist and Radiologist imaging physicians, other solutions must be pursued in parallel. Artificial intelligence (AI) is prevalent within non-cardiac Radiology workflows and to some degree within CVI workflows. However the accuracy and reproducibility within cardiac workflows is more challenging given the complexity of CVI and the field must ensure that before AI adoption in the attempt to improve efficiency, that further overburdening CVI physicians with verifying AI workflows does not occur in which case no true increase in efficiency would be achieved.
The development of new training statements is struggling to keep pace with the evolution of the field. As an example of the rapid knowledge increase in the field, a Pubmed search of “multimodality cardiac imaging” demonstrates an increase in publications from 8 in 2004 to 1,617 in 2024, a greater than 20,000% increase in 20 years. After training is completed, continued training occurs rapidly on the job through a variety of resources; however, due to the exponential increase in information, ongoing education remains a significant challenge.
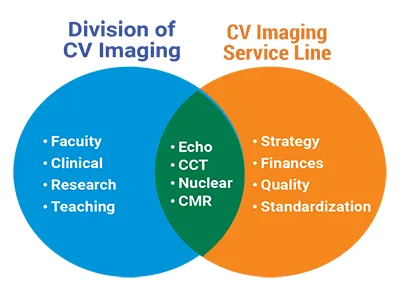
Traditionally, the subspecialities organized within Cardiology include Interventional, Electrophysiology, and Heart Failure & Transplantation. Newer models include Adult Congenital Heart Disease (overlap with Pediatric Cardiology) and Preventive Cardiology. Organization of the CVI modalities within a dedicated Division of Cardiovascular Imaging (DCVI) is a preferred method of solidifying this field into a recognized subspecialty of Cardiology within institutions. The CVI physicians work within the DCVI in their clinical, research, and teaching roles. In parallel, a Cardiovascular Imaging Service Line (CVISL) can be developed which includes management of all of the CVI modalities across hospital and ambulatory locations within a health system. The leadership who governs the service line is responsible for overseeing and implementing strategic, financial, and quality initiatives for the CVISL.
The DVCI/CVISL is a more efficient way of handling these initiatives and eliminating traditional silos within CVI. The CVISL model also facilitates incorporation of the significant technical resources necessary for the innovation heavy CVI space. Other unique aspects of the CVISL result from the involvement of Cardiologists and/or Radiologists who perform clinical CVI reading services. The CVISL is integrated as part of the overall Cardiovascular Service Line, which improves its efficiency and connection to the main service line. With center specific governance councils, Cardiology imaging physicians, Non-imaging Cardiologists (including but not limited to general, electrophysiologists, interventionists, and heart failure cardiologists) and dyad administrators would be important leaders. Radiologists, where applicable, could also be part of the membership of the CVISL if needed as they are important stakeholders in reading non-cardiac findings and possibly CVI studies as well depending on local operations. However, in newer models where the CVISL is incorporated within the CVSL, the governance council mainly consists of cardiovascular specialists.

Needs for the future revolve around attracting trainees to the field, balancing efficiency with quality, and optimizing reimbursement. Attracting new trainees should start in general cardiology fellowship where current exposure is extremely limited. A significant increase in the number of training slots is needed. While newer generation trainees are attracted to the technology and noninvasive aspects of CVI, higher salaries and CVI dedicated practice patterns will be required for retention in the field. Volumes are outpacing the rate of new hiring and resources, and thus improvements in AI to reduce the CVI workload and maintain quality will be additive. Furthermore, efforts legitimize the field as an accredited subspeciality and advocacy work will be needed to improve salaries to reflect the significant extra training and expertise required to produce high quality and accurate results.
References
1. Edler I, Hertz CH. The use of ultrasonic reflectoscope for the continuous recording of the movements of heart walls. 1954. Clin Physiol Funct Imaging 2004;24:118-36.
2. Kuhl DE, Edwards RQ. Cylindrical and Section Radioisotope Scanning of the Liver and Brain. Radiology 1964;83:926-36.
3. Hounsfield GN. Computerized transverse axial scanning (tomography). 1. Description of system. Br J Radiol 1973;46:1016-22.
4. Nutt R. 1999 ICP Distinguished Scientist Award. The history of positron emission tomography. Mol Imaging Biol 2002;4:11 26.
5. Lauterbur PC. Image formation by induced local interactions. Examples employing nuclear magnetic resonance. 1973. Clin Orthop Relat Res 1989:3-6.
6. Cribier A, Eltchaninoff H, Bash A et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation 2002;106:3006-8.
7. Hahn RT. The new paradigm for the management of valvular heart disease: the multi-disciplinary heart team. J Am Soc Echocardiogr 2011;24:A28.
8. Leipsic J, Wood D, Manders D et al. The evolving role of MDCT in transcatheter aortic valve replacement: a radiologists' perspective. AJR Am J Roentgenol 2009;193:W214-9.
9. Beller GA. A proposal for an advanced cardiovascular imaging training track. J Am Coll Cardiol 2006;48:1299-303.
10. Sayed A, Al Rifai M, Alwan M et al. Cardiac Imaging Trends: A Decade of Medicare Data. JACC Cardiovasc Imaging 2025;18:511-513.
11. https://medicushcs.com/resources/an-inside-look-at-the-cardiology-workforce-shortages-demand-and-strategic-responses.
12. https://medicushcs.com/resources/the-radiologist-shortage-addressing-the-gap-between-supply-and-demand.
13. Garcia-Sayan E, Jain R, Wessly P, Mackensen GB, Johnson B, Quader N. Radiation Exposure to the Interventional Echocardiographers and Sonographers: A Call to Action. J Am Soc Echocardiogr 2024;37:698-705.
14. Mehta LS, Lewis SJ, Duvernoy CS et al. Burnout and Career Satisfaction Among U.S. Cardiologists. J Am Coll Cardiol 2019;73:3345-3348.
15. Narula J, Chandrashekhar YS, Dilsizian V et al. COCATS 4 Task Force 4: Training in Multimodality Imaging. J Am Coll Cardiol 2015;65:1778-85.
16. Choi AD, Thomas DM, Lee J et al. 2020 SCCT Guideline for Training Cardiology and Radiology Trainees as Independent Practitioners (Level II) and Advanced Practitioners (Level III) in Cardiovascular Computed Tomography: A Statement from the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr 2021;15:2-15.
17. Little SH, Rigolin VH, Garcia-Sayan E et al. Recommendations for Special Competency in Echocardiographic Guidance of Structural Heart Disease Interventions: From the American Society of Echocardiography. J Am Soc Echocardiogr 2023;36:350-365.

Dr. Omar Khalique, MD, FACC, FSCCT, FASE, FSCMR, FSCAI is the Director of the Division of Cardiovascular Imaging at St. Francis Hospital and Catholic Health in Long Island, New York. Dr. Khalique is a recognized international expert in the fields of Multimodality Cardiovascular Imaging and Structural Heart Disease Imaging.
