Hospital partnership programs that connect High-Income Countries (HICs) with Low- and Middle-Income Countries (LMICs) are redefining the future of global surgery. Going beyond technology transfer, these programs enable scalable training models, foster innovation, and empower local healthcare teams. One such example is the partnership between Germany’s Hospital Partnerships program and Rural Surgery Innovations in India. This article explores how such collaborations have not only improved surgical access but also driven systemic change—through low-cost innovation, simulator-based learning, and cross-border mentorship.
Global surgery has long faced the challenge of bridging the access gap between well-resourced and underserved regions. While infrastructure and workforce limitations persist, a new paradigm is emerging—one driven not merely by financial aid but by strategic partnerships rooted in mutual learning, innovation, and local empowerment.
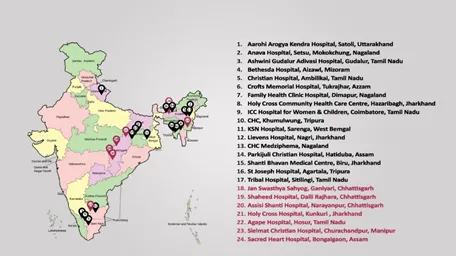
The Hospital Partnerships program, funded by Germany’s Federal Ministry for Economic Cooperation and Development (BMZ) and supported by GIZ, exemplifies this shift. Partnering with the German Society for Tropical Surgery (DTC) and Rural Surgery Innovations in India, the project aimed to bring Minimally Invasive Surgery (MIS) capabilities to rural hospitals. Initially scoped to train 12 surgeons across six hospitals, the program dramatically exceeded expectations—ultimately reaching 64 surgeons across 17 rural hospitals. This article examines the cascading impact of this collaboration and the systemic insights it offers into sustainable global health interventions.
1. Training Beyond the Target
Indicator: Number of rural surgeons trained
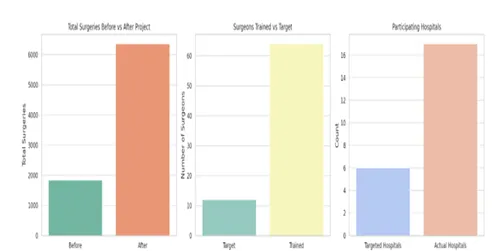
Outcome: A total of 64 rural surgeons received training—far surpassing the original goal of 12. This reflects not only effective outreach but also a keen demand among rural clinicians for advanced surgical skills.
2. Widening the Institutional Footprint
Indicator: Number of participating hospitals
Outcome: 17 rural hospitals were empowered with new MIS capabilities, greatly expanding the geographic footprint of surgical access.
3. Population Impact
Indicator: Population with increased access to surgical care
Outcome: Immediate catchment populations totaled 547,630, with extended populations approaching 2.77 million. This positions the partnership as a significant enabler of regional health equity.
4. Surgical Volume: A Leap in Capability
Indicator: Surgical procedures performed
Outcome: Yearly surgeries rose from 1,844 to 6,363—a 3.5x increase, signifying not just improved skills but enhanced patient throughput and confidence.
5. Dramatic Improvements in Surgical Coverage
Indicator: Procedures per 100,000 population
Outcome:
Overall coverage across the project area jumped from 580 to 2,148 surgeries per 100,000—highlighting a transformation in rural surgical capacity.
6. Multi-Disciplinary Capacity Building
Indicator: Total doctors and nurses trained
Outcome: 51 doctors and 172 nurses received training, with 60 reporting enhanced surgical skills. This represents systemic strengthening of care teams—not just individual capacity-building.
7. Mentorship and Proctorship as Enablers
Indicator: Onsite mentoring visits
Outcome: Proctorship visits averaged three per hospital, ensuring that hands-on support continued beyond initial training, reinforcing retention and confidence in real-world application.
The Hospital Partnership project generated several insights that could shape future global surgery collaborations:
1. Hospitals Invested in Their Own Progress
Contrary to expectations, most hospitals preferred to procure essential MIS equipment with their own funds rather than rely on the program. Only two of the 17 hospitals utilised project money for purchasing the Gas Insufflation-Less Laparoscopic Surgery (GILLS) device. This reflects a strong sense of local ownership—critical for sustainability.
2. Surging Demand for MIS Training
The original scope of 12 surgeons expanded to 64—indicating a widespread interest among rural clinicians in mastering minimally invasive techniques. This demand provides a compelling case for further investment in scalable training models.
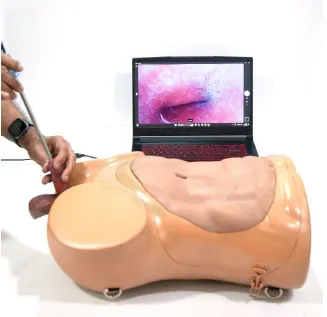
3. Simulator-Based Training: A Game-Changer
Realistic surgical simulators, developed during the project, enabled accelerated learning. Training durations were reduced, and surgeons could perform procedures shortly after simulator sessions. In Malawi, for example, trainees conducted laparoscopic procedures within a day of simulation-based training—despite having no prior hands-on exposure.
4. Organic Program Continuity
The program continued to expand even after the formal project period ended. Additional hospitals have joined the training network, demonstrating the viral nature of well-supported, peer-driven training ecosystems.
5. Funding Gaps for Human Resources
While equipment and travel costs were relatively easy to cover through hospital or local funding, paying for project staff remained a major challenge. This highlights a funding blind spot: operational sustainability often hinges on the ability to retain skilled coordinators and trainers.
Flexibility in Fund Reallocation
Success hinged on the ability to reallocate funds based on emerging needs. As more hospitals joined the training effort, budgets initially designated for equipment were repurposed for travel, while hospitality was often provided by the host institutions. This adaptability enabled scale without excessive overhead.
Geographic and Functional Scalability
The project scaled horizontally across Indian rural hospitals and extended internationally to Malawi—demonstrating a model that is both replicable and geographically flexible.
Continuous Monitoring and Feedback
Frequent reviews and agile course correction ensured that the project remained responsive and adaptive. This feedback loop is a hallmark of successful global health interventions.
1. Staff Compensation and Continuity
While local resources often cover infrastructure and consumables, sustained human resource support—particularly for trainers and coordinators—is difficult to fund post-project. Future iterations should include structured “exit grants” or wind-down salaries to ensure long-term continuity.
2. Equitable Access to Innovation
The project’s reliance on low-cost, innovative technologies (e.g., GILLS) demonstrates how appropriate tech can bridge the affordability gap. However, ensuring equitable distribution remains a priority—especially in more remote or underfunded hospitals.
3. Integration vs. Dependency
The aim is to create self-sustaining ecosystems rather than depend on ongoing external support. Simulator-based training and local mentorship are key enablers here—but must be complemented with scalable systems for accreditation and follow-up.
As Hospital Partnerships evolve, this project offers a working blueprint for similar collaborations. Key pathways forward include:
Hospital partnerships are no longer just channels for aid; they are frameworks for shared growth. This project exemplifies how collaborative models—backed by innovation, flexibility, and a deep respect for local agency—can transform rural healthcare ecosystems.
As we imagine the future of global surgery, programs like these serve as powerful reminders: the right partnerships, rooted in humility and mutual respect, can unlock capabilities far beyond the initial scope. The path to sustainable health equity lies not in charity—but in collaboration.

Dr. Gnanaraj Jesudian is a Urologist and General Surgeon from CMC Vellore who has been serving in rural and remote areas for over four decades. He has contributed to more than 100,000 surgical procedures and pioneered the introduction of minimally invasive surgery (MIS) in 78 rural hospitals. He has received multiple innovation awards, including the DST-Lockheed Martin Award, GE Healthcare Award, and Millennium Alliance Award. Dr. Jesudian is currently working on Gas Insufflation-Less Laparoscopic Surgeries and Laptop Cystoscopies—both of which are listed in the WHO Compendium of Innovative Health Technologies. He has over 425 publications with more than 890 citations. He serves as the Secretary of the IFRS, is a past President of ARSI, and sits on the Board of Directors of the G4 Alliance.
Dr. Henning Mothes is a specialist in Surgery, Trauma Surgery, and Specialised Visceral Surgery, with a diploma in Tropical Medicine and Public Health. He completed his surgical training at the University Hospital Jena and currently serves as the Chief Physician of the Department of General, Visceral, and Vascular Surgery at Weimar Hospital. He is also the President of the German Global Surgery Organisation (DTC).

Dr. Florian Graz is a Medical Doctor and Advisor in the Hospital Partnerships Programme at the German Agency for International Cooperation (GIZ). He oversees the Latin America portfolio and leads strategic cross-cutting initiatives, including innovation and digital health, to foster sustainable partnerships in global health cooperation.
