Artificial intelligence and digital health technologies are transforming cardiology by enabling a shift from reactive, hospital-centred care to preventive, participatory, predictive and personalised medicine. Despite advances, cardiovascular disease remains the leading global cause of death, with persistent sex differences in diagnosis and outcomes. AI-driven analytics and digital tools offer new opportunities to address these gaps and advance precision medicine.
Cardiovascular disease(CVD) remains the leading cause of mortality in both men and women worldwide. For decades, CVD was largely perceived as a predominantly male condition. Clinical paradigms, diagnostic thresholds, and therapeutic strategies were largely developed and validated in male populations. As a result, women’s CV health has remained under-recognised and understudied despite overwhelming evidence that CVD is the leading cause of death in women globally.
Women differ from men not only in CV anatomy and physiology but also in pathophysiology, age at disease onset, symptom presentation, CV risk factors, diagnosis, and management strategies. Some conditions, such as microvascular angina, spontaneous coronary artery dissection, and myocardial infarction with non-obstructive coronary arteries (MINOCA, INOCA), disproportionately affect women and often evade traditional diagnostic frameworks. Furthermore, gender related factors, including caregiving responsibilities, socioeconomic disparities, and implicit bias in healthcare interactions, compound these differences.
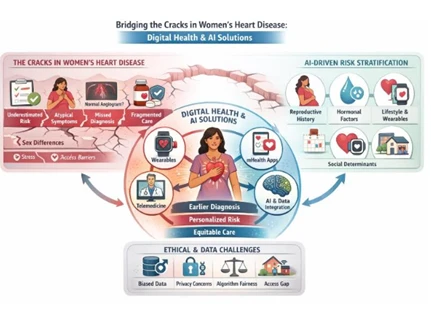
The term cracks in women’s heart disease refers to these systemic failures: delayed diagnosis, misclassification of risk, insufficient representation in clinical trials, underdiagnosis, undertreatment, and worse prognosis. Addressing these cracks requires more than incremental improvements it demands a paradigm shift. At this point, digital health Technologies and AI are uniquely positioned to drive this transformation.
2.1 Diagnostic Gaps and Atypical Presentation
Women experiencing acute/chronic coronary syndromes frequently present with symptoms that deviate from the classic ‘’crushing chest pain’’ paradigm. Shortness of breath, fatigue, nausea, epigastric discomfort, back pain, and anxiety are commonly reported. These atypical presentations often lead to misinterpretation, delayed triage, and underuse of noninvasive/ınvasive diagnostic tools.
Traditional diagnostic tools also perform differently in women. Electrocardiographic changes may be subtle, troponin thresholds may be sex dependent, treadmill ECG changes may be misleading, SPECT results may be false negatives, and coronary angiography may reveal nonobstructive disease despite ongoing ischemia. Consequently, women are more likely to be discharged without a definitive diagnosis, reinforcing a cycle of undertreatment.
2.2. Limitations of traditional risk stratification
Widely used CV risk models, such as Framingham Risk Score or Score fail to incorporate female-specific risk enhancers or fail to take the impact of classical risk factors on coronary arteries into account. Besides pregnancy-related complications (such as gestational hypertension, preeclampsia, and gestational diabetes), premature menopause, autoimmune diseases, and psychosocial stressors are either underweighted or entirely absent from these models.
This leads to systematic underestimation of CV risk in women, particularly younger women and those without traditional risk factors. As a result, preventive therapies are often initiated too late.
2.3 . Underrepresentation in clinical research
Women remain underrepresented in CV clinical trials, accounting for approximately 25-35% of participants. Even when included sex specific analyses are inconsistently reported. This data gap limits the generalizability of evidence-based guidelines and perpetuates uncertainty regarding optimal therapies for women.
Digital health encompasses a broad ecosystem of tools, including wearable devices, mHealth applications, telemedicine platforms, and Electronic health records. Together, these technologies enable continuous real-world data collection and patient-centered care models.
3.1 Wearable Technologies and Continuous Monitoring
Wearable devices such as smartwatches and biosensors have transformed CV monitoring from episodic snapshots to continuous streams of physiological data. Parameters such as heart rate, heart rate variability, physical activity, sleep patterns, rhythm irregularities, and blood pressure recordings can now be tracked longitudinally.
Beyond advantages for both sexes, these technologies offer extra advantages for women, such as:
Continuous monitoring also validates women’s symptoms by providing objective physiological correlates, helping counteract the dismissal of subjective complaints.
3.2 Mobile Health Applications and Symptom Tracking
Mobile health applications empower women to actively engage in their cardiovascular care. Symptom diaries, medication reminders, lifestyle coaching, and educational content can be tailored to women’s needs and life stages.
Importantly, structured symptom tracking enables the capture of atypical and fluctuating symptom patterns that are often missed during brief clinical encounters. When integrated with clinical workflows, these data enhance shared decision-making and diagnostic accuracy.
Artificial intelligence, particularly machine learning and deep learning, excels at identifying complex, non-linear patterns in large datasets. In women’s cardiovascular health, AI has the potential to reveal insights that traditional statistical approaches overlook.
4.1 AI in Cardiovascular Diagnosis
AI-enhanced analysis of electrocardiograms, echocardiography, cardiac MRI, and CT imaging can detect subtle features associated with ischemia, cardiomyopathies, and microvascular dysfunction, which is prominent in women. AI-driven natural language processing (NLP) can also extract clinically relevant information from unstructured medical notes, capturing symptom narratives often underappreciated in women.
By integrating multimodal data, AI systems can reduce diagnostic uncertainty and shorten time to diagnosis—critical steps in closing gender gaps in acute and chronic care.
4.2 Personalised Risk Prediction
AI-based risk models can incorporate a wide range of variables, including reproductive history, hormonal status, psychosocial stress, wearable-derived metrics, and social determinants of health. This holistic approach enables personalised, sex-sensitive risk stratification across the lifespan.
For women, such models may identify elevated cardiovascular risk years before traditional scores signal concern, enabling earlier preventive interventions.
5.1 The Data Problem
Artificial intelligence is only as good as the data on which it is trained. Current cardiovascular datasets are often:
As a result, AI models developed using such datasets may perpetuate or even amplify algorithmic bias, leading to reduced accuracy and reliability of predictions for women.
5.2 Ethical and Data Security Considerations
Several ethical and safety issues require particular attention when applying AI in women’s cardiovascular health, including:
Failure to adequately address these concerns may undermine patient trust and exacerbate existing health inequities.
6.1 Women-Specific Algorithms
Developing women-centered AI models requires:
Such approaches enable more accurate and personalised cardiovascular care for women.
6.2 Clinical Decision Support Systems
AI-powered clinical decision support systems can assist clinicians by providing real-time alerts, such as:
These alerts have the potential to reduce diagnostic delays and improve clinical decision-making.
6.3 Remote Monitoring and Reducing Health Inequities
For women living in rural areas or with limited access to healthcare services, digital health solutions offer substantial opportunities, including:
Together, these strategies can help reduce geographic and socioeconomic disparities in women’s cardiovascular care.
As explained till now, heart disease in women requires special attention. The persistent gaps often described as the cracks in women’s heart disease are rooted in biological sex differences, gender related social factors, and long-standing biases in clinical research and healthcare systems. Digital health Technologies and AI offer unprecedented opportunities to identify, quantify, and ultimately bridge these gaps.

Nurgül Keser, MD, is a Professor of Cardiology at Health Sciences University. She graduated from Istanbul University Faculty of Medicine in 1992 and completed her cardiology residency at Cerrahpaşa Faculty of Medicine in 1997. She also completed a research fellowship in echocardiography at the University of Alabama at Birmingham under Prof. Navin C. Nanda. Dr. Keser founded a Women and Health Research Center, co-edited Heart Disease in Women, and serves on international editorial boards. She is CEO of SUN Healthcare, with a focus on artificial intelligence, digital health, women’s cardiovascular disease, hypertension, heart failure, and multimodal imaging.
