An Australian public health reflection from Monash Health on lessons learned from the Covid-19 pandemic. We discuss the public health strategies to help stop the “infodemic”, crucial elements for a health programme to be successful, Australian national Covid-19 response framework and what the very important lessons are learned from our own experiences fighting the pandemic. With an uncertain future short and long term priorities are addressed.
First of all, I would like to thank the editorial office of the AmericaHHM Magazine for inviting me to this editorial interview which covers this very current and still challenging topic of Covid pandemic. I studied medicine both in US and Europe after which I entered general surgery and cardiothoracic surgical residency in Berlin, Germany. Additional training in heart and lung transplant with German Heart Institute in Berlin where I spent my initial 2 years working as a consulting surgeon before moving to the Alfred Hospital Cardiothoracic and Transplant Services in Melbourne, Australia. Spent considerable time in research as well, mainly associated with transplant surgery and basic science. Further interests in minimally invasive cardiac procedures, aortic surgery and surgery for heart arrhythmias. Always had interest in public health and epidemiology which I treated as my hobby in medical domains. As the Covid pandemic hit in early 2020, I decided to step aside and join Victorian Department of Health in a public health officer and mentor role. It was a very challenging period for myself and all my much more experienced colleagues at the Department. I used that period to additionally advance and educate myself in Public Health and Medical Administration and commenced MBA with La
Trobe University as well. After spending 18 months with Department of Health Victoria in Melbourne, I was offered a public health role at the newly formed Monash Health Public Health Unit in Oct 2021, which covers the whole south east of Melbourne approx. 3.5 million residents. I am currently involved in developing strategies and management of residential age care facilities in this area.
It’s a very difficult question which we all in public health and wider are trying to tackle, but in my opinion it starts from every individual and everyone counts. I would have few suggestions for your readership.
The new Delphi Covid consensus, which was just published, the volume and velocity of information during the COVID-19 pandemic has made it difficult for individuals to evaluate the accuracy of any given piece of information. When public health officials' communications fail to accurately reflect the reality that SARSCoV-2 transmission is largely airborne, they regrettably contribute to the spread of incorrect information. Additionally, governments have handled erroneous information in the COVID-19 pandemic context in an inconsistent manner. There are undoubtedly a lot of places where misleading information may be found, which weakens the social cohesiveness required for effective public health responses. The public health officials had engaged populations with low levels of immunity ineffectively as the pandemic was starting to spread.
This is just a slide that represents these crucial elements for an effective and successful public health program and was developed by Australian Federal Department of Health with our collaboration from Melbourne and Victoria. I am always using it as a starting point.
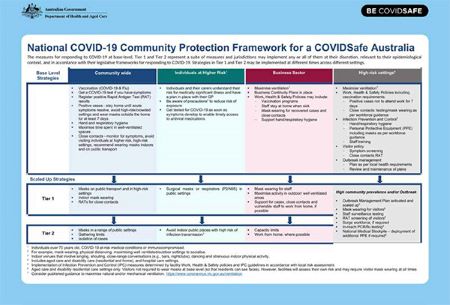
It only took few months early in the Covid-19 pandemic 2020 to develop this very simple and flexible plan that proved to be very successful over last few years.
As you can see the very essence of this framework is the fundamental base level strategies in community settings, individuals at higher risk, business sector, and high risk settings being accordingly adjustable in Tier 1 and 2 scaled up options when required.
So having a national community based framework not only to deal with the current Covid-19 pandemic but for all the potential future pandemics and crisis situations is one of the crucial elements for a public health response and programme to be successful.
Further to that I would like to emphasize that health systems are continuing to face enormous staffing shortages mainly to do with the mental and physical health impacts on their workers from the pandemic. Healthcare workers continue to experience unaddressed mental health issues due to protracted working hours and increased risks in healthcare settings. Governments have not always addressed the high out-ofpocket expenditure to consumers for some pandemic control measures (for example, testing) and personal protective equipment (for example, facemasks). The COVID-19 pandemic continues to reveal vulnerabilities in the global supplychain framework for essential public health supplies. The COVID-19 pandemic has catalysed opportunities for rapid innovation in digital health solutions throughout the care continuum.
During public health emergencies like the global Covid-19 outbreak, managing regional economies of scale and scope using internationally pooled procurement can unquestionably assist health services in enhancing access to necessary medications and supplies.. Community-based interventions and services to address pandemic-related issues continue to be underused by healthcare providers in many countries.
As recent research has indicated that when the risk of harm to others is increasingly prevalent, the authorities may determine that the right of all citizens to good health overrides the autonomy of any one individual who chooses not to be involved in the vaccination program. As we are aware that medical autonomy acknowledges that every person who has decision-making capacity has the right to make decisions regarding their treatments and immunization, even when their decisions may contradict their health providers’ recommendation and support. Despite the availability of immunization services, vaccine reluctance—which can range from postponing to outright rejection—remains a significant obstacle to managing the COVID-19 pandemic as a hazard to public health in every nation.
The main emphasis of future responses should concentrate on how to improve and strengthen our public health systems and collaborate accordingly not only on a local level but much wider to easier exchange and disseminate the critical scientific data flow. These are some of the facts learned through the pandemic which I will further elaborate on.
Healthcare providers and systems have experienced wide-ranging challenges throughout the Covid pandemic, from periods of relative calm and control to periods of struggle and near collapse. Although many healthcare systems will continue to be at risk of being overtaken by the new waves, the unanimous agreement among the Covid Delphi consensus panellists strongly implies that those risks may be addressed and mitigated. The absence of an evidence-based data, a globally accepted platform of minimal COVID-19 pandemic response recommendations and standards is one of several factors that endanger health systems in a structural manner. While the community transmission of SARS-CoV-2 still continues to havoc around the world and create risks to health systems, especially through variants of concern, robust virological surveillance should be implemented in all areas.
Given the persisting uncertainties regarding the prevalence, virulence, severity, and duration of post-COVID-19 morbidity due to extended Covid, pertinent public health strategies should better account for the possible longterm implications of undetected transmissions of COVID-19. In order to deliver improved public health and clinical targets relating to the COVID-19 pandemic, all member nations should give the World Health Organization (WHO) the go-ahead. This endeavour should focus especially on cases, immunisation rates, morbidity, and mortality. Massive economic impact, particularly expenditures borne by consumers and businesses, raises the stakes for the health care system.
Removing financial obstacles to COVID-19 tests, personal protective equipment, medical treatment, and patient care are just a few of the risks that should be addressed with strong structural and economic recommendations. There should also be a clear plan to support the establishment of local and regional production hubs for COVID-19 supplies, medications, and vaccines, as well as the necessary legislative and regulatory changes and reforms to address market weaknesses and risks. Authorities and healthcare professionals should think about using a flexible approach in nations where access to PCR or fast antigen tests is inadequate or constrained. The duties of primary healthcare should be enhanced and properly supported in order to lessen the impact and load on hospitals, and the physical, mental, and social wellbeing of the healthcare workforce should also be improved.
The recommendations should stimulate expanding IT infrastructure expenditures, further modifying and enhancing user interfaces, and efforts to widen access, especially for vulnerable demographic groups and individuals. Digital health will play an additional significant role. Investing in the development of applications and platforms to identify the best digital health solutions Relevant public health policies should better take into account the potential long-term effects of undiscovered COVID-19 transmissions given the ongoing uncertainties surrounding the prevalence, virulence, severity, and duration of post-COVID-19 morbidity caused by extended Covid. All members should grant the World Health Organization (WHO) the go-ahead in order to meet better public health and clinical aims related to the COVID-19 pandemic. Particular attention should be paid to cases, immunisation rates, morbidity, and mortality in this endeavour.
Significant economic impact raises the stakes for the healthcare system, especially when it comes to costs incurred by consumers and corporations. In order to address all of these issues, strong structural and economic recommendations should remove financial barriers to Covid-19 tests, personal protection equipment, medical treatment, and patient care. They should also have a well-defined strategy for how ideas may be quickly expanded and supported.
So besides the traditional issues like an ageing population and increasing demand on health services. Increasing rates of chronic disease. Costs of medical research and innovations the Australian health landscape has been immensely affected by covid-19 pandemic since early 2020. Although Australian health system is considered one of the best in the world, the covid pandemic has exposed number of deficiencies and gaps in the system and just confirmed that even with the best planning, vulnerabilities are very hard to foresee, especially when you are dealing with a very novel and invisible enemy.
In terms of medication and pharma supply issues, Australia imports approximately 90% of its medicines from China and India, while the locally produced medications and their producers have traditionally had to compete with offshore companies on costs and logistics, raising recent concerns that Australia is ‘dangerously dependent’ on global supply chains. NPS Medicine Wise has estimated more than nine million Australians are being prescribed daily medications, which means that medical providers need to more closely and frequently follow up patients’ health conditions considering the current shortage of medications on our market.
The TGA (Therapeutic Goods Administration) stipulates that many disruptions can’t be avoided, admitting that the issue of drug supply shortages is not unique to Australia. Further factors contributing to short supplies include manufacturing problems, difficulties in procurement, overseas political instability, global market crises, the current pandemic, and natural disasters in other regions. It’s just unfortunate that the current situation leaves patients with no alternative but to pay additional costs for essential medication or adjust their dose until they can be provided with their correct medications, with shortages at local pharmacies being a daily struggle. That means marked-up prices on generic brand medications, and pharmaceutical companies ringing overseas suppliers to outsource critical medications. Luckily these issues and concerns have been already dealt with in Australia and the local supply chains have been increasingly popping up and covering the existing gaps in manufacturing domains. We can only see the global surge on local supply and manufacturing capabilities in the next decade, that’s where significant investments are being diverted.

Many of us through the Covid pandemic have admitted that we all have recognized and unrecognized weaknesses, but resilience and adaptability emerged as one of our main strengths. With recognized weaknesses, it’s much easier to deal with and plan, or do risk management modelling. While the main burning issues might be different elsewhere, I see and recommend to other healthcare systems and providers to try and recognize what potential team weaknesses might be in their setting and environment. Running regular assessment modellings for a specific health provider or area is one of the tools available.
We certainly think that further improvements in essential medical infrastructure and resource checks can be very challenging but are necessary. As we have experienced that despite the fact that the healthcare system in normal conditions, providing general medical services, and lacking Covid trained staff and appropriate PPE equipment, including doctors, nurses, and other emergency staff, but with proper plan and management and the use of enthusiastic young and skilled healthcare workers, was able to maintain treatment management indicators, such as doctor and nurse-to patient ratios, and more importantly ventilator-to-population ratio, almost close to our standards. With appropriate use of hospital capacities space, additional number of beds, and necessary equipment were also created in the main Covid wards.
Additional capacities to treat Covid patients were also created in other healthcare settings and emergency departments. With good communication and team building strategies like regular meetings, motivation team huddles, and peer support of the healthcare management teams in the fight against Covid- 19 we have been able to address and deal with our weaknesses, becoming stronger, and more resilient and ultimately improving our response to the pandemic. For the leadership teams the importance of regular weekly meetings, brainstorming of ideas to improve the response, further discussing operational plans in various areas of health were usually held with the presence of hospital administrators, public health officers and other decision-makers to evaluate the implementation of newly developed protocols and strategies.
Primary directions for Monash will be governed by our mid and long term plan which has that flexibility in the case of need. As we see the very turbulent economic crisis at the moment, war in Ukraine and lots of challenges managing covid-19, I think that future investments will be in local manufacturing of essential medical consumables, strategic stockpiling, relying on local energy resources and transitioning to self sufficient health systems which will be able to survive longer periods of time on their own resources. Further transition to health digitalisation and patient communication platforms, digital public health systems and teaming up with start-ups in relevant domains. Vaccine production facilities like the current collaboration between Monash Health, Moderna and Victrian Department of Health to support the production facility in Melbourne. So I see a lot of new changes in a very short future, further collaborations between the healthcare providers globally will be of huge financial benefits.
That was very tough as most health providers in Australia had to completely cancel or reschedule even life-saving surgeries and procedures. We obviously had to adapt quickly and develop strategies with the collaborative approach with our inter state and federal colleagues and health providers. So re assessing all our lists on regular basis and involving the primary health care providers who played an amazing role as well. Between the initial restrictions and free periods we increased the number of procedures to compensate for the periods lost, emergency and high priority patients were never cancelled and we always found the solutions necessary to get the things done. The resilience played a great role and the general population was very understanding a tolerable considering the situation, lots of going into the communities and talking to them.
We learned on the job what our short and longterm priorities are through the initial support and recommendations of The Australian Commonwealth government postulated healthrelated actions during the primary response to the Covid-19 pandemic: provides national leadership in managing external borders and protecting residents of aged care facilities and approves, procures, and rolls out multiple vaccine options.
The initial short-term priorities were very effective and could be always readily re-implemented again. Our state governments were responsible for determining what public health measures are appropriate, adopting emergency response legislations and implementing them promptly—with managing the border quarantine arrangements and the required Covid testing, tracing, and isolation protocols, with additional management of healthcare and hospital response. As it has been over three years of fragmented but coordinated global and national responses, we can certainly advocate noting that three of the highestranked recommendations call for the adoption and implementation of whole-of-society and whole-of-government models, while proven prevention measures using an Covid-19 immunization approach that incorporates a wide range of public health and financial support measures to additionally compliment the vaccination programs. Long term priorities would be to monitor the situation and develop more flexible public health response strategies as we really don’t know when the next pandemic may hit back and please remember that it may not be related to Covid or one of its variants. Obviously we have learned a lot and probably desire more credit than we realize. We were very vulnerable initially but resilient and quicky learned to adapt as a society on a global level. I still have to acknowledge the positive role Chinese healthcare workers played at the very start of the pandemic, it’s sad that they are not properly recognized as they were at the forefront and only took them few weeks to share the genomic sequence of the Covid-19 virus. This has been unfortunately politicized a lot around the world, precious time was lost and some countries are still talking about it.
It’s very hard to foresee the future and especially with Covid-19 being so adaptable and variant prone virus. For myself personally I do intend to further contribute to public health and stay in some capacity at Monash Health, although my next endeavour might be in research and clinical work, so I will try to be involved on multiple fronts of challenging medical and public health issues. I look forward to complete the necessary transitions of public health response in age care facilities which at the moment take most of my time. We should be a better and safer place in 5 years from now and I can see the changes and improvement literary on a daily basis. Hopefully we can say that for many other regions in the world as well. Who knows we may touch base again in 5 years and reflect? Time will only tell.

An internationally recognised cardiothoracic surgeon and public health officer who joined the Covid19 public health response in Melbourne, Australia. After having spent initial 18 months of pandemic, working with Victorian State Department of Health he joined Monash Public Health Unit which took over the Covid-19 management in southeastern Melbourne suburbs.





