Medical record completeness is crucial for patient care, but the audit process still has a lot of waste. The clinical and quality assurance algorithm integration with structured medical record data is the new approach to a completely lean process, a reduction in error, and real-world improvement in patient care.
Why do hospitals have to audit their medical records regularly, and why is it important?
As we all know, data in medical records plays a crucial role in patient care, process management, and risk management, particularly legal risk management. Moreover, all hospital quality accreditation standards, both local—such as Thai Hospital Accreditation (HA)—and global—such as Joint Commission International (JCI) and Global Health Accreditation (GHA)—emphasize the importance of medical record completeness and issue specific auditing guidelines. Not only in the hospital, but external parties such as payors, the government, and the private sector also pay attention to the data in the medical record. Hence, its completeness affects hospital revenue as well.
Although hospital executives and staff fully acknowledge the importance of complete medical records, the comprehensive medical record audit process remains unsatisfactory and needs to be improved. Most hospitals in Thailand still have issues with medical records, as shown below:

The above pain points come from several reasons, some of which are external and uncontrollable factors, such as unclear and variable audit standards. Most standards identify concepts, e.g., "appropriate" or "sufficient," that need further interpretation. For example, "When appropriate, the family’s educational needs of each patient are assessed and recorded in the patient’s medical record." Therefore, misinterpretation among auditors may occur. Each hospital's quality accreditations and payer standards have similar or different perspectives. If hospitals use many accreditations, some audit items may conflict with each other or become redundant, causing auditing to be unclear or auditors to become confused. However, the following internal factors are possible to control and improve:to control and improve:

To overcome these challenges, this topic will demonstrate the new approach that totally disrupts the existing medical record audit method, starting from setup to implementing medical record audit logic with IT integration as follows:
1. Standard review: All medical record audit items of all accreditation standards must be reviewed and consolidated by qualified persons who profoundly understand the objectives of the standard. Moreover, knowledge and experience in hospital management, medical care, and hospital context would be helpful. The reviewer must identify which items are related to the organization and compare similarities across standards; then, the duplicate items must be removed. From this step on, the single list of medical audit items will be ready
2. EMR field review and audit item mapping: Every EMR screen should be reviewed and mapped with the audit items. This process will be more convenient if the EMR field has identified standard terminology, e.g., SNOMED-CT, Medcin. As for hospitals that use paper-based medical records, the new approach will be impossible. Although HIS in electronic form is already in place, HIS's cooperation is still the biggest challenge. A separate clinical documentation software that already labels standard terminology is a suitable alternative method.
3. Convert a standard into programming logic: If the identified EMR field is a custom code, terminology may be required during an audit of the programming logic conversion. This step is the most challenging because programmers should also have clinical and hospital quality assurance knowledge.
4. User interface development: The audit score, missing element list, and recommendation is helpful for real-time feedback. These could be either pop-ups or links to the full report. The key consideration for the development is "real-time," allowing effective chart review and complete correction before finalizing the document. A fundamental tool for developing these features will likely be available for the modern EMR.
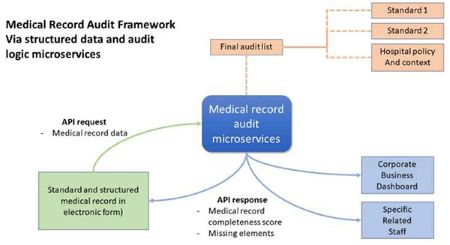
5. Monitoring tool development: The dashboard supports executives, the quality management team, and the business unit. It also performs other functions. Committees can access details of the audit results in real-time. The feedback can also reach individual staff, including a doctor, who plays a critical role in medical record completeness. The developer's skill to create a dashboard is not a big challenge because several business intelligence tools are available nowadays. The key success factor is dashboard design. The chart data, type, layout, and analytic design should be done by someone experienced in quality assurance because this is an important part of hospital accreditation. After complete setup and development, as in other new technology implementations, the hospital will face challenges related to changed management and the variety of user skills and knowledge. Effective communication and training will always be the key success factors. Before everyone recognizes the outcome, like increased medical record completeness, the users will perceive several better experiences, such as:
Bangpakok 9 Hospital is an excellent example of successfully implementing this medical record audit approach in a very short period of time. The key success factors are strong governance and management with clear directions that aim to improve the quality of care using lean management. The organizational culture of this hospital also supports consistent electronic medical record usage and user familiarity with digital adoption. Moreover, they wasted no time on audit rule review or logic development. The easiest way to implement this approach is by using ready-to-use microservices for medical record audit that comply with the local standard (hospital accreditation, or HA) and global standard (Joint Commission International, or JCI). With an instantly calculated audit score, the opened chart review percentage increased from 20% to 100%.

Piyanun Yenjit is a country manager of HIMSS Thailand and founder of APUK, a healthcare digital transformation consultant and microservices provider, focusing on improvement in patient safety, process efficiency, and business growth. She is also experienced in electronic medical records with structured data implementation compatible with various quality assurance standards.





